Thyroplasty ( Medialization laryngoplasty) – What is it?
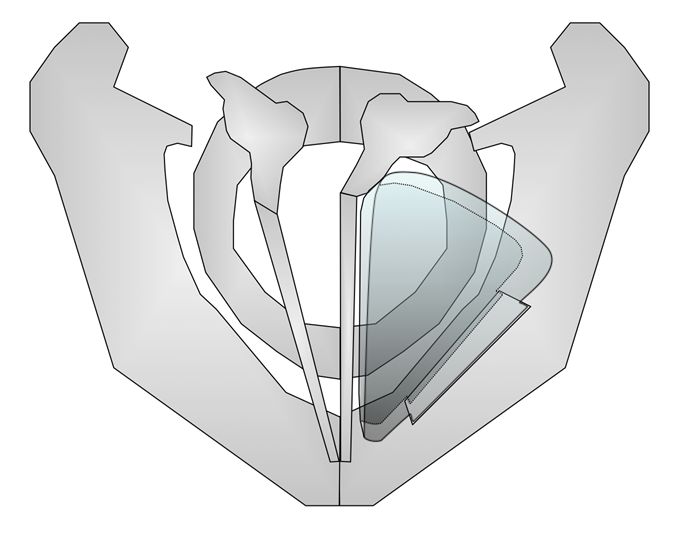
Permanent vocal fold medialization can also be achieved by surgery on the neck from the outside. For this purpose, an opening (“window”) is made in the thyroid cartilage at the level of the paralyzed vocal fold, into which an implant is inserted, thereby pushing the vocal fold toward the center. The operation can be performed under anesthesia or local anesthesia. Various implants are available, including titanium braces, prefabricated silicone wedges, custom-configured silicone wedges, and GoreTex strips. Some surgeons choose autologous cartilage. Usually, this procedure is performed during an inpatient stay. Since this surgery interferes with the cartilage framework of the larynx, it belongs to the so-called “Laryngeal Framework Surgery”. After hundreds of thyroplasties, we have had the best experience with our individually intraoperatively fabricated silicone implants.
Thyroplasty – In which cases it is applied
Medialization thyroplasty (thyroplasty for short) is indicated in cases of inadequate closure of the glottis. This is usually the case with unilateral vocal cord paralysis, but also with voice-enhancing surgery after tumor treatment. This can be the case after recurrent nerve paralysis, chordectomy after tumor operations of vocal fold(s), presbylarynx, vocal fold bowing, and other disorders.
This voice enhancement surgery involves a permanent shift of the vocal fold to the middle by inserting an implant from the outside. This procedure often requires an inpatient stay.
We mostly use a special technique with preoperative 3D-scanning of the larynx with a cone beam imaging technique, the digital volume tomography (DVT). We can then apply a computer aided design (CAD) of the ideal implant size and form.